
Care Designed Around Recovery, Not Reimbursement
Peak Body & Mind is a direct-pay psychiatric practice in Reno, Nevada. We opted out of insurance because the treatments that produce real, measurable recovery for treatment-resistant depression, PTSD, postpartum depression, and cognitive decline - ketamine, peptides, IV nutrient therapy, neuroregulatory injections, and objective brain testing - sit entirely outside the insurance formulary. This page examines the reimbursement system, the evidence behind standard-of-care prescribing, and exactly what direct payment buys you.
The System Is Not Built FOR YOU
The current mental health system was built to process volume, not to heal. Insurance-based psychiatry was architected around billing codes, 15-minute medication checks, and whatever treatment costs the least to reimburse - not whatever treatment works best.
The result is a system in which providers are financially penalized for spending time with patients, reimbursed for the cheapest possible intervention, and structurally prohibited from offering anything outside a narrow formulary of approved treatments whose patents expired before most of their patients were born.
Behavioral health providers are reimbursed at rates approximately 22% lower than equivalent medical and surgical services, creating a direct financial incentive to minimize complexity, minimize time, and minimize the depth of care a patient receives. That is not a flaw in the system. It is the system.
We opted out of that system - not because billing is complicated, but because staying in it would mean practicing a version of medicine we don't believe in.
We built Peak Body & Mind on a different premise: that the biological underpinnings of mental illness are identifiable, measurable, and correctable. When you address them directly - with the right tools, the right sequence, and the right clinical rigor - people get better in ways standard psychiatric care cannot reliably produce.That work cannot be done in 15 minutes. It cannot be billed to a plan that doesn't recognize it. And it cannot happen inside a system that was never designed to support it.
The System Was Designed FOR EFFICIENCY Not Healing.
Insurance-based psychiatry was built to process volume, not to treat the root cause.

BILLING CODES
Care is shaped by what can be coded, not what is clinically needed.
15-MINUTE VISITS
Short appointments make complex problems impossible to solve.
LOWEST COST TREATMENTS
Reimbursed for the cheapest option, not the most effective.
MEDICATION FIRST
A narrow formulary of old drugs becomes the default.
SYMPTOM MANAGEMENT
The focus is on managing symptoms, not resolving causes.
Providers are financially penalized for doing what healing requires.
Clinicians who slow down to treat the whole person are penalized, while quick, surface-level care is rewarded.
LOWER REIMBURSEMENT
for behavioral health providers
Compared to equivalent medical and surgical services.
This creates a financial incentive to minimize complexity, time, and depth of care.
Two Different Models. Two Different Outcomes.
THE CURRENT MODEL
Insurance driven
Limited time
Limited options
Reactive care
Symptom suppression
THE PEAK MODEL
Patient centered
Extended evaluations
Precision diagnostics
Root cause approach
Lasting transformation

We chose to leave that system.
BIOLOGY IS REAL
Mental illness has biological underpinnings that are measurable and correctable.
.png)
THE RIGHT TOOLS
When you treat the cause, not just the symptoms, people actually get better.
.png)
ROOT CAUSE MATTERS
Advanced testing and clinical precision reveal what standard care consistently misses.
.png)
THE RIGHT SEQUENCE
Healing follows a sequence.
We address foundations before symptoms.
.png)
BETTER OUTCOMES
Our approach leads to results standard psychiatric care cannot reliably produce.
MENTAL HEALTH IS BIOLOGY
When biology improves,
the mind often follows.
-Photoroom.png)
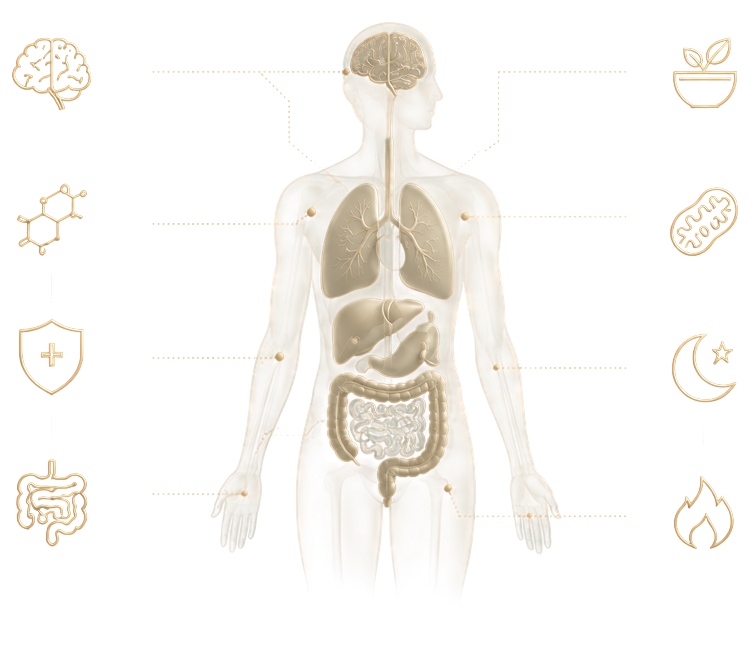
BRAIN CHEMISTRY
HORMONES
IMMUNITY & INFLAMMATION
GUT HEALTH
NUTRITION
MITOCHONDRIA & ENERGY
SLEEP
METABOLISM
That work cannot be done in 15 minutes. It cannot be billed to a plan that doesn't recognize it. And it cannot happen inside a system that was never designed to support it.
.svg)
We built Peak Body & Mind on a different premise:
that the biological underpinnings of mental illness are identifiable, measurable, and correctable. When you address them directly - with the right tools, the right sequence, and the right clinical rigor - people get better in ways standard psychiatric care cannot reliably produce.
Insurance Doesn't Cover What Actually Works
The treatments with the strongest emerging evidence for treatment-resistant depression, PTSD, postpartum depression, and cognitive decline are, almost without exception, outside the scope of what insurance will reimburse:
IV Ketamine
the only treatment with rapid-onset antidepressant effects validated across multiple randomized controlled trials for TRD - is not covered.
IV nutrient therapy
which addresses the mitochondrial and NAD+ deficits that drive anhedonia and cognitive impairment, is not covered.
Compounded peptide therapies
with documented effects on neuroinflammation, BDNF production, and HPA normalization are not covered.
Objective brain-function assessment
via quantitative EEG and somatosensory metrics is not covered.
The stellate ganglion block
a sympathetic nerve procedure with published evidence for PTSD - is not covered.
This is not a coincidence; it is an economic reality. Insurance systems reimburse treatments that are cheap to administer, easy to standardize, and profitable to pharmaceutical manufacturers.
Treatments that are biologically sophisticated, individualized, or that compete with reimbursable drugs don't survive the approval process - not because they don't work, but because the system was never designed to evaluate them fairly.
To be direct: most of what happens at Peak Body & Mind, insurance wouldn't cover regardless. This isn't a practice that went direct pay to avoid paperwork. The treatments that produce results here - ketamine, peptides, IVNT, neural therapy, neuroregulatory injections - don't exist on any formulary.
Direct pay isn't a workaround; it's the only structure in which this medicine can be practiced honestly.
Patients who rely exclusively on insurance-covered psychiatric care are, by structural necessity, limited to treatments already selected against innovation.
They're offered the cheapest available option and told it's the best one. Those two things are not the same.
Mental illness is a biological problem. It has biological drivers, biological signatures, and biological solutions. The system built to treat it was designed around none of those facts - it was designed around reimbursement schedules, formulary politics, and administrative efficiency.
Choosing direct pay psychiatric care is not choosing luxury. It is choosing a different standard - one that starts with "What is actually happening in this patient's biology?" rather than "What does the plan cover?" Those two questions lead to very different clinical decisions, and over a treatment relationship, very different outcomes
We didn't build Peak Body & Mind to be the convenient option. We built it to be the right one.
The Honest Case
References
[1] Melek S et al. Addiction and Mental Health vs. Physical Health. Milliman, 2017.
[2] SAMHSA. Key Substance Use and Mental Health Indicators in the United States. 2022.
[3] Rush AJ et al. STAR*D Report. Am J Psychiatry. 2006.
[4] Kirsch I et al. Initial Severity and Antidepressant Benefits. PLoS Med. 2008.
[5] Moncrieff J et al. The serotonin theory of depression. Mol Psychiatry. 2022.
[6] Uher R et al. An inflammatory biomarker as a differential predictor. Am J Psychiatry. 2014.